
Giant Papillary Conjunctivitis (GPC)
An allergic-type reaction causing bumps under the eyelids, often from contact lens wear. Learn about causes, symptoms, and management.
Giant papillary conjunctivitis (GPC) is an inflammatory condition of the inner surface of the upper eyelid, characterized by the formation of large bumps called papillae. It's most commonly associated with contact lens wear but can occur with any foreign material that contacts the eye repeatedly. GPC causes itching, mucus discharge, and lens intolerance.
Key Takeaways
- Inflammatory reaction on the underside of upper eyelid
- Most common cause: contact lens wear (especially soft lenses)
- Main symptoms: itching, mucus discharge, lens discomfort
- Treatment: lens discontinuation, anti-inflammatory drops, lens modifications
- Often recurs if contact lens habits don't change
- Not an infection—it's an immune/mechanical reaction
What Causes Giant Papillary Conjunctivitis?
GPC is caused by a combination of chronic mechanical irritation and immune response, most commonly from contact lens wear. Protein and lipid deposits on lenses, lens edge irregularities, and overwearing lenses trigger an inflammatory reaction on the underside of the upper eyelid.
The Underlying Mechanism
GPC involves both mechanical irritation and immune response:
- Chronic friction against the inner eyelid
- Immune reaction to deposits on contact lenses
- Combination of Type I (immediate) and Type IV (delayed) hypersensitivity
- Results in papillae (bumps) formation on tarsal conjunctiva
Common Triggers
Contact Lens-Related (Most Common)
- Soft contact lenses (especially extended wear)
- Lens deposits (protein, lipid)
- Lens edge irregularities
- Poor lens hygiene
- Overwearing lenses
Other Foreign Bodies
- Exposed sutures after eye surgery
- Ocular prosthetics (artificial eyes)
- Scleral buckle components
- Extruded hardware
What Are the Risk Factors for GPC?
The biggest risk factor for GPC is soft contact lens wear, especially extended-wear lenses that are not replaced frequently enough. People with allergic tendencies, poor lens cleaning habits, and longer total duration of lens wear are also at higher risk.
- Soft contact lens wear (higher risk than rigid)
- Extended wear lenses (higher risk than daily)
- Infrequent lens replacement
- Poor lens cleaning habits
- Allergic tendencies (atopy)
- Environmental allergies
- High protein tear film
- Longer duration of lens wear (years)
What Are the Symptoms of Giant Papillary Conjunctivitis?
GPC symptoms develop gradually and progressively worsen over time. Early signs include mild itching and lens discomfort toward the end of the day. As the condition advances, mucus discharge increases, lenses become intolerable, and vision may blur from mucus on the lens surface.
Progressive Symptoms
Early Stage:
- Mild itching after lens removal
- Slight increase in mucus
- Lenses feel less comfortable toward end of day
- May be asymptomatic
Moderate Stage:
- Significant itching (during and after wear)
- Increased mucus, especially in morning
- Lens awareness throughout the day
- Lens movement increases
- Blurred vision from mucus
Severe Stage:
- Unable to tolerate contact lenses
- Significant discharge
- Lenses displace with blinking
- Constant foreign body sensation
- Lid heaviness or ptosis (drooping)
What You Might Notice
- White or clear stringy mucus, especially upon waking
- Itching that's worse when wearing lenses or just after removal
- Feeling like something is in the eye
- Needing to remove lenses earlier in the day
- Lenses moving too much or popping out
- Foggy or filmy vision
How Is Giant Papillary Conjunctivitis Diagnosed?
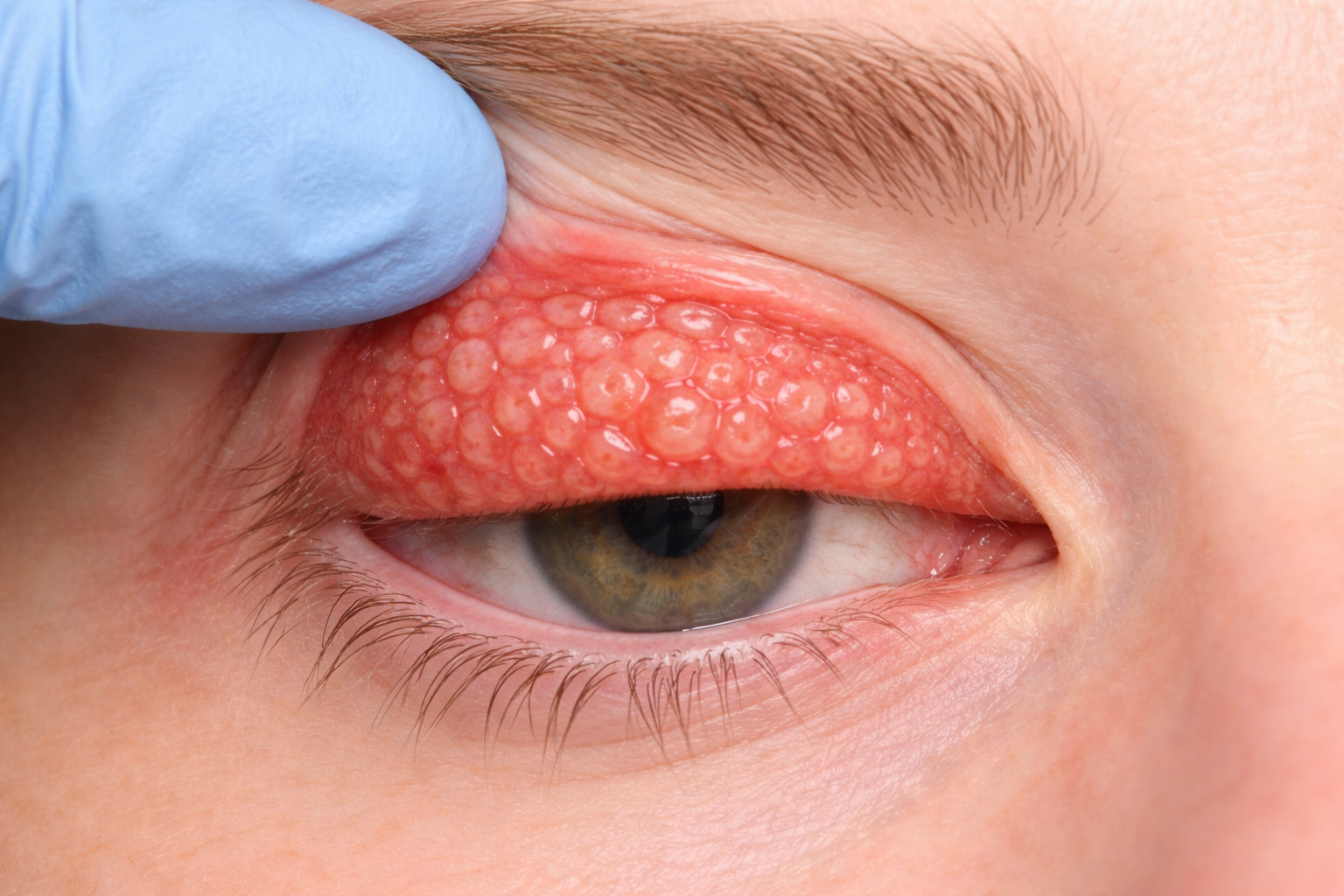
Diagnosis requires flipping the upper eyelid to examine its inner surface. The doctor looks for raised bumps (papillae) on the tarsal conjunctiva—"giant" papillae are larger than 0.3 mm, and severe cases show a distinctive cobblestone appearance greater than 1 mm.
Clinical Examination
Diagnosis requires examining the underside of the upper eyelid (everting the lid):
What the Doctor Sees:
- Papillae (raised bumps) on upper tarsal conjunctiva
- "Giant" papillae are > 0.3 mm in diameter
- In severe cases, papillae may be > 1 mm ("cobblestone" appearance)
- Mucus strands
- Redness of the lid lining
Grading
| Grade | Papillae Size | Symptoms |
|---|---|---|
| 1 (Mild) | 0.3-0.5 mm | Minimal symptoms |
| 2 (Moderate) | 0.5-1.0 mm | Moderate itching, mucus |
| 3 (Severe) | > 1.0 mm | Significant symptoms, lens intolerance |
Differential Diagnosis
- Allergic conjunctivitis
- Vernal keratoconjunctivitis
- Atopic keratoconjunctivitis
- Infectious conjunctivitis
For a broader look at conditions that mimic pink eye, see our guide on conditions mistaken for pink eye.
How Is Giant Papillary Conjunctivitis Treated?
The most important step is reducing or eliminating the trigger—usually contact lens wear. Treatment then involves anti-inflammatory medications to resolve the papillae, followed by careful modifications to lens type, care regimen, and wearing habits before returning to contacts.
Step 1: Discontinue or Modify Lens Wear
The most important step is reducing or eliminating the trigger.
- Complete lens discontinuation may be needed initially
- Duration depends on severity (days to weeks to months)
- This allows the papillae to resolve
Step 2: Medical Treatment
Mast Cell Stabilizers/Antihistamines:
- Olopatadine (Pataday, Pazeo)
- Ketotifen (Zaditor)
- Azelastine (Optivar)
- Used daily to reduce inflammation and itching
For Moderate to Severe Cases:
- Short-term topical steroids (loteprednol, fluorometholone)
- Used under doctor supervision
- Tapered as papillae improve
Supportive:
- Cool compresses
- Artificial tears
- Lid hygiene
Step 3: Contact Lens Modifications
When returning to lens wear:
Lens Material Changes:
- Switch to daily disposable lenses (best option)
- Consider rigid gas permeable (RGP) lenses
- Try different soft lens materials
- Avoid silicone hydrogels if problematic
Care Regimen Changes:
- Switch to hydrogen peroxide disinfection system
- More frequent lens replacement
- Better cleaning compliance
- Reduced wearing time
Prevention of Recurrence
- Use daily disposable lenses when possible
- Replace lenses on schedule (don't overwear)
- Proper lens cleaning and care
- Limit wearing hours
- Regular eye exams
- Continue prophylactic antihistamine drops if needed
If your eye symptoms keep returning despite these measures, see our guide on recurring pink eye for other potential causes.
When Can You Return to Contact Lens Wear?
The timeline for returning to contacts depends on the severity of GPC. Mild cases may allow a return in days to weeks with modifications, while severe cases may require months off lenses. Some patients cannot return to soft contact lenses at all.
Timeline
- Mild GPC: May resume with modifications in days to weeks
- Moderate GPC: Usually need weeks off lenses
- Severe GPC: May need months; some can't return to soft lenses
Best Practices for Return
- Wait until papillae have resolved (confirmed by exam)
- Start with new, fresh lenses
- Use daily disposables if possible
- Limit initial wearing time (build up gradually)
- Use prophylactic antihistamine drops
- Follow up regularly
Don't resume lens wear without doctor clearance.
Returning to lenses too soon or without modifications often leads to rapid recurrence, sometimes worse than before.
What Are the Alternative Vision Correction Options?
If GPC keeps recurring despite modifications, several alternatives to soft contact lenses are available. These range from glasses and rigid gas permeable lenses to permanent solutions like refractive surgery.
If GPC recurs despite modifications:
- Glasses—always an option
- Rigid gas permeable lenses—less likely to cause GPC
- Orthokeratology—worn only at night
- Refractive surgery (LASIK, PRK)—eliminates need for contacts
What Is It Like Living with GPC?
With proper management, most people with GPC can continue wearing some form of contact lenses successfully. Daily disposable lenses dramatically reduce recurrence, though you may need to limit wearing time and be more vigilant about lens hygiene than the average wearer.
Daily Management
- Pay attention to comfort—don't push through discomfort
- Remove lenses at first sign of problems
- Keep antihistamine drops available
- Don't sleep in lenses (unless specifically designed for this)
- Handle lenses with clean hands
Long-Term Outlook
- Most people can return to some form of contact lens wear
- Daily disposables dramatically reduce recurrence
- Some need to limit wearing time permanently
- A minority cannot tolerate soft contacts at all
- Regular monitoring helps catch recurrence early
When Should You See a Doctor for GPC?
See an eye doctor if you're experiencing increasing lens discomfort, mucus discharge, or reduced wearing time with your contact lenses. Don't try to push through symptoms—continuing to wear lenses without modification can worsen the condition and prolong recovery.
See a doctor if:
- Contact lenses are becoming increasingly uncomfortable
- You notice white or clear stringy mucus, especially in the morning
- Lenses are moving excessively or popping out
- Vision is foggy or filmy while wearing lenses
- You need to remove lenses earlier in the day than usual
- Itching persists after lens removal
- You've been diagnosed with GPC before and symptoms are returning
Frequently Asked Questions
Will GPC go away on its own?
If you continue wearing contact lenses the same way, GPC typically worsens. Discontinuing lens wear allows improvement, but modifications are needed to prevent recurrence when returning to lenses.
Can I just switch to a different brand of contacts?
Sometimes switching lens types helps, but often additional measures (daily disposables, better care, reduced wear time, medications) are needed. Simply changing brands without other modifications often fails.
Is GPC an allergy?
GPC involves immune mechanisms similar to allergies (hence the itching and response to antihistamines), but it's primarily triggered by mechanical irritation and lens deposits rather than environmental allergens.
How do I know if my GPC is better?
Symptoms improve (less itching, less discharge), and your doctor can confirm by examining your upper eyelids. Don't assume you're better just because symptoms are mild—the papillae need time to resolve fully.
Will I always have this problem?
With proper management (daily disposable lenses, good hygiene, possibly prophylactic drops), most people can continue wearing contact lenses successfully. However, you'll likely remain predisposed and need to be more careful than the average lens wearer.
References
Medical Disclaimer: This information is for educational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have contact lens-related eye problems, please consult a qualified healthcare provider.
Sources:
- American Academy of Ophthalmology. Giant Papillary Conjunctivitis.
- Donshik PC. Giant papillary conjunctivitis. Trans Am Ophthalmol Soc. 1994;92:687-744.
- Skotnitsky CC, et al. General and local contact lens associated papillary conjunctivitis (CLAPC). Clin Exp Optom. 2006;89(4):193-197.
- American Association for Pediatric Ophthalmology and Strabismus. Allergic Conjunctivitis.