
Pink Eye in Children
Learn about pink eye in kids — how to identify the type, when antibiotics are needed, safe home care, school return policies, and when to call the doctor.
Pink eye is one of the most common reasons children miss school—and one of the most common reasons parents call the pediatrician or eye doctor. While most cases of childhood conjunctivitis are mild and self-limiting, knowing which type your child has determines whether they need antibiotics, how to manage symptoms at home, and when they can go back to school.
Key Takeaways
- Viral conjunctivitis is very common in school-age children and does not need antibiotics
- Bacterial conjunctivitis causes thick yellow-green discharge and responds to antibiotic drops or ointment
- Allergic conjunctivitis causes intense itching, affects both eyes equally, and is not contagious
- Most schools require 24 hours of antibiotic treatment before a child can return (for bacterial cases)
- Home care with compresses, artificial tears, and lid hygiene is safe and effective for most mild cases
- Newborn eye discharge is always urgent—see a doctor immediately
Why Pink Eye Is So Common in Children
Children are particularly susceptible to pink eye for several reasons:
- Close contact in schools and daycare spreads infection rapidly
- Frequent face and eye touching — children are less aware of hygiene
- Shared toys and objects in classroom settings
- Developing immune systems — less resistance to new viruses and bacteria
- Nasolacrimal duct issues — young children may have incomplete drainage systems
Pink eye causes substantial school absenteeism in the United States each year, according to CDC conjunctivitis data.
Types of Pink Eye in Children
Viral Conjunctivitis
Very common in school-age children and usually caused by adenoviruses (bacterial conjunctivitis is more common in preschool-age children):
- Watery, clear discharge
- Often starts in one eye and spreads to the other
- May accompany a cold, sore throat, or ear infection
- Highly contagious — spreads easily in classrooms
- Resolves on its own in 1–3 weeks
- Antibiotics won't help
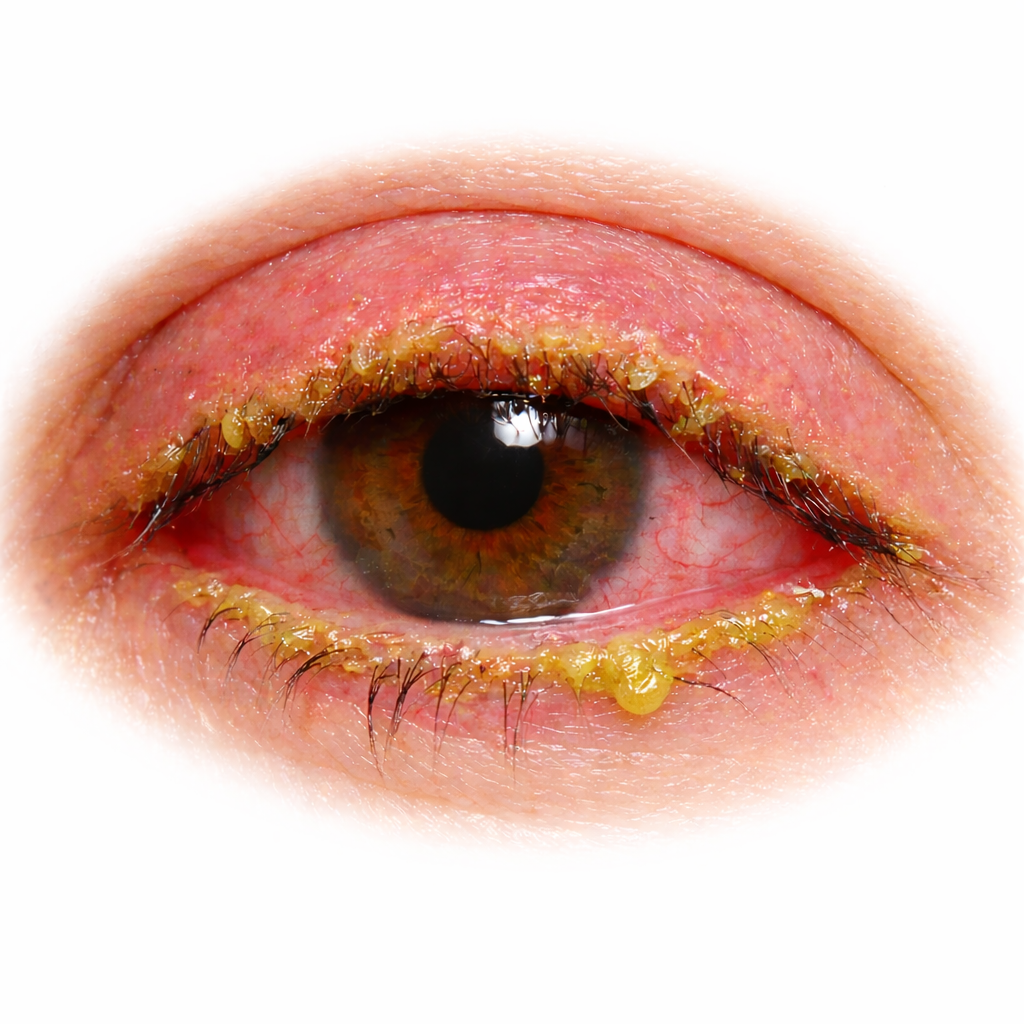
Bacterial Conjunctivitis
More common in younger children (especially preschool age):
- Thick, yellow-green discharge
- Eyelids stuck together in the morning
- Often caused by Haemophilus influenzae, Streptococcus, or Staphylococcus
- Responds well to antibiotic drops or ointment like erythromycin ointment
- Contagious until 24–48 hours after starting antibiotics
Allergic Conjunctivitis
Common in children with allergies, asthma, or eczema:
- Intense itching — the hallmark symptom
- Both eyes affected equally
- Clear, stringy discharge
- Seasonal pattern or triggered by pet exposure
- Not contagious — no need to miss school
- Responds to antihistamine drops
What to Look For
Signs your child may have pink eye:
- Red or pink appearance of one or both eyes
- Discharge — watery, mucous, or thick and colored
- Eye rubbing — children may rub eyes frequently
- Complaining of itching, burning, or "something in my eye"
- Eyelids stuck shut in the morning (bacterial)
- Swollen eyelids
- Tearing
- Light sensitivity
How to check: Gently pull down the lower eyelid to look for redness of the conjunctiva. Note the type of discharge — watery suggests viral or allergic; thick and colored suggests bacterial. Check both eyes, even if only one looks affected.
Home Care for Children
For All Types
- Wash your hands before and after touching your child's eyes
- Use clean, damp washcloths to gently wipe away discharge
- Don't let your child share towels, pillowcases, or washcloths with siblings
- Wash bedding and towels in hot water
- Encourage your child not to touch or rub their eyes
For Viral Pink Eye
- Cool compresses for comfort (10 minutes, several times daily)
- Preservative-free artificial tears for soothing
- No antibiotics needed
- Keep your child home while symptoms are worst (first 3–5 days, though they may remain contagious for up to 2 weeks)
For Bacterial Pink Eye
- Warm compresses to loosen morning crusting
- Gentle lid hygiene to clean discharge
- Apply prescribed antibiotic drops or ointment as directed
- Complete the full course even if symptoms improve quickly
Tip for applying eye drops in children: Have your child lie down with eyes closed. Place the drop in the inner corner of the eye. When they open their eyes, the drop rolls in. For ointment, pull down the lower lid and apply a thin ribbon.
For Allergic Pink Eye
- Cool compresses for itch relief
- Over-the-counter antihistamine drops (ketotifen—safe for ages 3+)
- Artificial tears to wash away allergens
- Have your child shower and change clothes after playing outdoors
- Keep windows closed during high-pollen days
For more home care strategies, see our pink eye home remedies guide.
When Antibiotics Are Needed
Antibiotics are appropriate for:
- Confirmed or strongly suspected bacterial conjunctivitis (thick, colored discharge)
- Moderate to severe cases — significant swelling, discomfort, or copious discharge
- School return — many schools require antibiotic treatment before readmission
- Children under 2 years with conjunctivitis — lower threshold for treatment
- Contact lens wearers (older children/teens) — to prevent complications
Antibiotics are not needed for:
- Viral conjunctivitis (the most common type)
- Allergic conjunctivitis
- Mild bacterial cases that are already improving
Don't pressure your doctor for antibiotics if they diagnose viral pink eye. Using antibiotics for viral infections doesn't help your child, contributes to antibiotic resistance, and exposes them to potential side effects. Viral pink eye simply needs time to resolve.
School and Daycare Policies
Policies vary, but typical guidelines include:
For bacterial pink eye:
- Most schools allow return 24 hours after starting antibiotic drops/ointment
- Discharge should be noticeably improving
- Some schools require a doctor's note
For viral pink eye:
- Guidelines vary widely — some schools require doctor clearance
- Generally, children can return once discharge has significantly decreased
- Strict hand hygiene should be maintained after return
For allergic pink eye:
- No restrictions — allergic conjunctivitis is not contagious
- If your child is sent home by mistake, a doctor's note can clarify the diagnosis
Tips for parents:
- Ask your school or daycare about their specific policy at the start of the year
- Get a doctor's note when possible to avoid confusion
- Explain to your child the importance of hand washing and not sharing personal items
For details on how long each type is contagious, see our guide on is pink eye contagious.
Preventing Spread in the Family
When one child has contagious pink eye:
- Separate towels and washcloths for the infected child
- Wash hands frequently — especially after caring for the child's eyes
- Clean toys that the infected child has touched
- Change pillowcases daily for the infected child
- Don't share eye drops between family members
- Disinfect surfaces the child frequently touches
- Watch siblings for early symptoms
Newborns: A Special Case
Neonatal conjunctivitis (eye discharge in the first 28 days of life) is an entirely different situation from pink eye in older children.
Any eye discharge in a newborn requires immediate medical evaluation.
Neonatal conjunctivitis can be caused by:
- Chemical irritation from birth prophylaxis (benign, resolves quickly)
- Gonococcal infection (can cause blindness within 24–48 hours)
- Chlamydial infection (can lead to pneumonia)
- Herpes simplex virus (can be life-threatening)
Do not attempt home treatment for newborn eye discharge. Seek care immediately.
When to Call the Doctor
Schedule an appointment if:
- Symptoms haven't improved after 3–5 days of home care
- Thick discharge persists despite warm compresses
- Your child needs clearance to return to school
- Symptoms keep recurring (see our guide on recurring pink eye)
- You're unsure whether it's viral, bacterial, or allergic
Seek same-day or urgent care if:
- Your child has significant eye pain (not just irritation)
- Vision seems affected — your child reports blurry vision or difficulty seeing
- Severe eyelid swelling — especially if the eyelid is red and warm (could be orbital cellulitis)
- A white spot is visible on the eye
- Your child wears contact lenses and has a red, painful eye
- Symptoms are worsening rapidly
- Your infant (under 1 year) develops eye discharge
Emergency signs in children:
- Severe eyelid swelling with fever — could indicate orbital cellulitis, which requires hospitalization
- Inability to open the eye due to swelling
- Any eye symptoms in a newborn
- Severe pain or sudden vision loss
Frequently Asked Questions
My child keeps getting pink eye. Why?
Frequent pink eye can result from ongoing allergen exposure, chronic blepharitis, nasolacrimal duct obstruction (blocked tear duct, common in infants), reinfection at school, or reinfection from contaminated items. If your child gets pink eye more than 2–3 times a year, see an eye doctor. See also our guide on how long pink eye lasts.
Can my child go swimming with pink eye?
No. Swimming can worsen symptoms and spread the infection to others. Wait until symptoms have fully resolved.
Is pink eye dangerous for children's vision?
Simple viral, bacterial, or allergic conjunctivitis almost never causes lasting vision problems. However, severe untreated bacterial infections, chronic inflammation, or complications like corneal ulcer can potentially affect vision. In rare cases, chronic visual deprivation in a young child can contribute to amblyopia. This is another reason to seek care for persistent or severe cases.
Can I use adult eye drops for my child?
Preservative-free artificial tears are generally safe for children. Antihistamine drops (ketotifen) are approved for children ages 3 and older. Prescription antibiotic drops should be used only as directed by your child's doctor. Never use "redness relief" drops in children.
Should I keep my child's siblings home too?
Only the child with contagious pink eye needs to stay home. Siblings without symptoms can attend school, but should practice careful hand hygiene and avoid sharing personal items with the infected child.
References
Medical Disclaimer: This information is for educational purposes only and does not replace professional medical advice, diagnosis, or treatment. If your child has eye symptoms, please consult a qualified healthcare provider.
Sources:
- American Academy of Ophthalmology. Conjunctivitis Preferred Practice Pattern.
- American Academy of Pediatrics. Pink Eye (Conjunctivitis).
- Rose PW, et al. Chloramphenicol treatment for acute infective conjunctivitis in children in primary care: a randomised double-blind placebo-controlled trial. Lancet. 2005;366(9479):37-43.
- Centers for Disease Control and Prevention. Pink Eye in Newborns.